
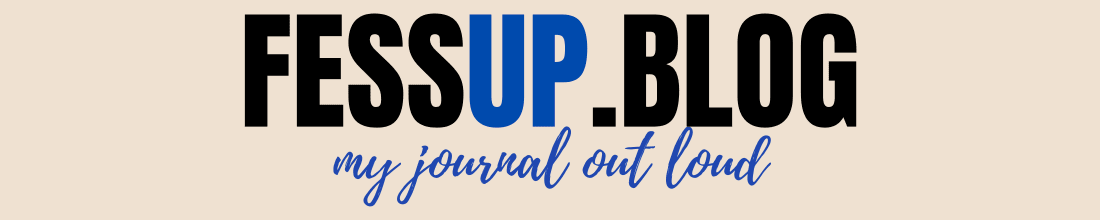
Under Observation
Trying to Stay Human in a Psych Ward

People talk about psychiatric hospitals like they are all one thing. Either they are life-saving sanctuaries full of compassionate professionals or they are nightmare institutions designed to strip people of their humanity.
My experiences taught me the truth is much less simple than either version.
I’ve been hospitalized in psychiatric units in my 20s, again in my 30s, and again in my late 40s. Some admissions genuinely helped me. Some left me feeling worse. I’ve had doctors who were brilliant, compassionate, and clearly exactly where they were meant to be. I’ve also encountered staff and providers who seemed burned out, dismissive, inexperienced, or completely unequipped to handle vulnerable human beings.
And honestly, a lot of the care you receive depends on why you are there in the first place.
Both times I was hospitalized as an adult were largely for medication management and rapid medication changes. That phrase alone probably sounds alarming to some people, and honestly, sometimes it should.
There are definitely situations where psychiatric hospitals become revolving doors. Someone survives a suicide attempt or reaches a breaking point, gets stabilized just enough to no longer be considered an immediate danger, and then gets discharged quickly because another person needs the bed. That reality exists. Pretending it doesn’t helps nobody.
But there are also situations where inpatient psychiatric care makes legitimate medical sense.
One time I was admitted because my doctors wanted to try an MAOI antidepressant. Because of the risks and interactions involved, they needed every trace of my previous antidepressants completely out of my system first. That meant stopping medications cold turkey and essentially rebooting everything under medical supervision.
And if you’ve ever abruptly stopped psychiatric medications, you already know that isn’t some casual process.
The hospitalization wasn’t because I was “crazy.” It was because the medication transition itself carried risks, and they wanted observation in case something went wrong physically or psychologically while my system adjusted.
That’s another thing people outside psychiatric care often don’t realize. Sometimes psych units are treating acute psychiatric crises. Other times they’re functioning almost like highly controlled medical observation units for the brain.
And depending on the hospital, the staff, and the level of competence involved, that experience can feel either incredibly supportive or deeply traumatizing.

The last time I was hospitalized, the experience was not therapeutic for me. It was frightening in a completely different way.
I was treated less like a person going through a specific medical and psychiatric situation and more like a generic “crazy person.” And honestly, there’s something deeply destabilizing about that.
Because once you’re inside a psychiatric unit, your normal reactions can suddenly be viewed through a distorted lens. If you’re upset, you’re “escalated.” If you’re frustrated, you’re “agitated.” If you strongly advocate for yourself, you’re suddenly “noncompliant.” After a while, you start feeling like you’re trapped inside someone else’s interpretation of you.
The closest thing I can compare it to is a kind of mistaken identity.
You know why you’re there. You know your own baseline. You know the situation is more nuanced than the chart in front of them. But suddenly you are inside a system responding to a version of you that doesn’t feel accurate at all. And that loss of control becomes terrifying because the people around you hold enormous authority over your treatment, your medications, your discharge, and even whether your emotions are considered reasonable.
Ironically, being constantly treated like you are irrational can become its own kind of psychological distress.
What made the experience especially difficult was that I was placed in a higher observation unit with people experiencing active suicidality, psychosis, or severe psychiatric crises, and I genuinely did not believe I belonged there.
The environment itself felt designed more for containment than healing.
You lose almost everything immediately. Your phone is taken away. Belts, shoelaces, ties, dental floss, anything remotely considered a risk gets removed. Contact with the outside world is reduced to payphone-style unit phones where you try to sound normal to worried friends or family while sitting under fluorescent lights surrounded by strangers in crisis.
Patients are monitored constantly. Cameras watch the unit and psych techs check rooms every fifteen minutes throughout the day and night. I understand why those precautions exist. For many patients, they are absolutely necessary. But when you already feel misplaced in that environment, the level of surveillance starts to feel wrong in a way you can’t quite argue your way out of.
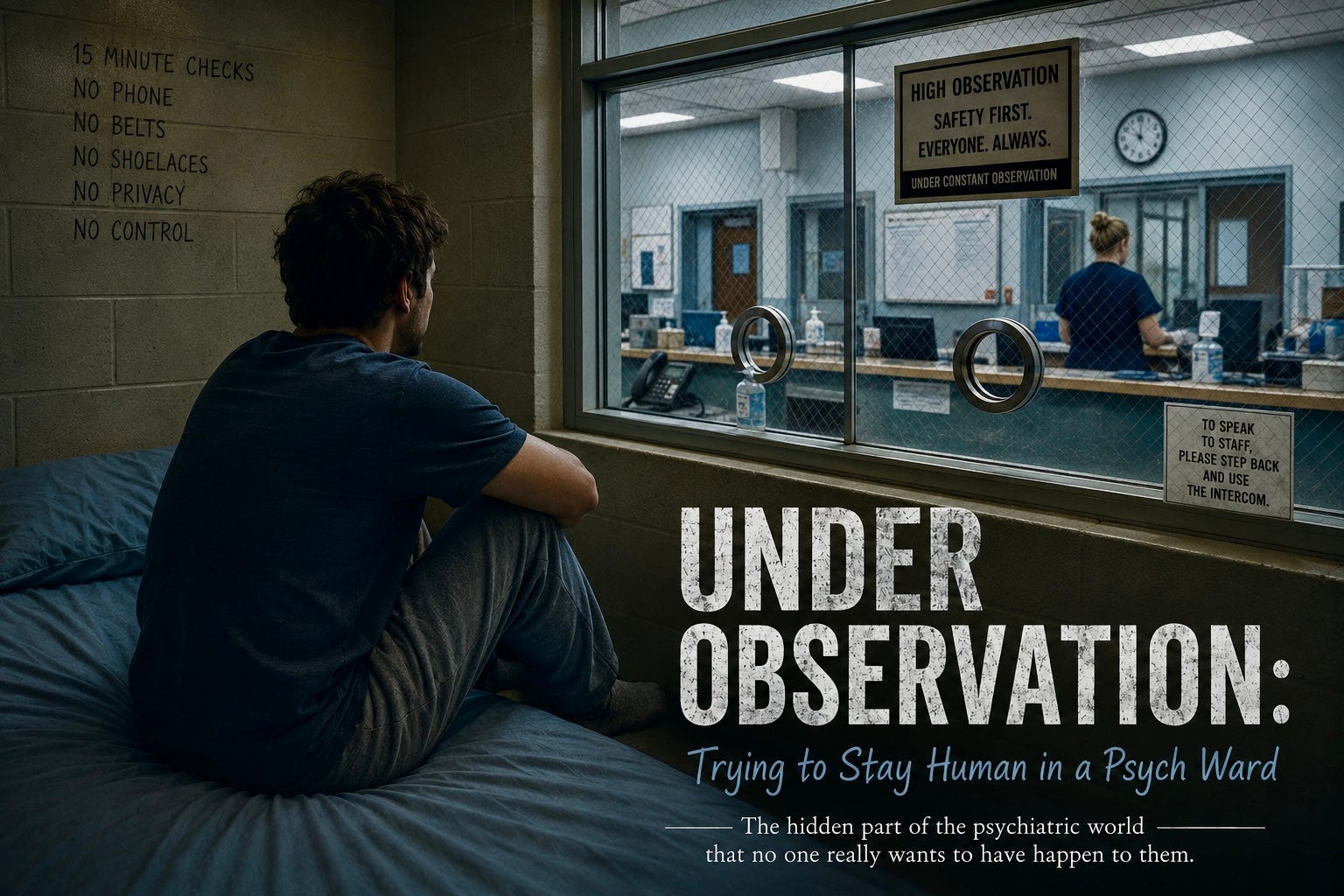
And in higher observation units, there is often another layer of separation that changes the emotional atmosphere completely: the staff themselves can feel physically inaccessible.
In the unit I was in, much of the nurses’ station was surrounded by protective glass. So even basic conversations sometimes happened through barriers that made the entire interaction feel more custodial than therapeutic.
Again, I understand why some of those precautions exist. Staff safety matters too, especially in units caring for patients in severe crisis.
But emotionally, it creates a strange dynamic.
When you are already frightened, overwhelmed, vulnerable, and questioning how people perceive you, speaking to nurses and staff members through protective glass can quietly reinforce the feeling that you are being viewed primarily as a potential threat instead of a person needing help.
It changes the atmosphere of the entire unit. The environment stops feeling relational and starts feeling institutional. Safe, maybe. Necessary for some situations, maybe. But still wrong in a way you can’t quite argue your way out of.
Sleep was almost impossible there, and one particular experience still stands out to me.
At the time, I had sleep apnea and used a CPAP machine. Because I was placed in the high observation unit, the machine’s power cord itself was considered a potential risk.
So every night, because the CPAP had to remain plugged in, they assigned someone to sit in my room and watch me while I slept to make sure I did not try to harm myself with the cord.
At least in theory.
In reality, having another person sitting in your room all night observing you is not exactly an environment that encourages sleep.
So I barely slept the entire time I was there.
And that’s part of what made the experience so disorienting. The unit was trying to keep people safe, but some of the precautions themselves became emotionally exhausting. Constant observation, constant noise, constant awareness that you are being monitored and assessed at all times. After a while, it stops feeling calming and starts feeling almost impossible to mentally settle inside your own body.
Anyone who has struggled with mental health already knows how deeply lack of sleep affects emotional regulation, anxiety, depression, and clear thinking. Yet somehow I was in an environment where rest felt nearly impossible.
And the physical design of the unit somehow made everything worse.
Ironically, it was a brand-new psychiatric facility, but it felt like nobody involved in designing it had ever actually asked psychiatric patients what helps people regulate emotionally.

There was no carpeting anywhere, so every footstep echoed. Every door creaked loudly. Conversations bounced off the walls. Nothing absorbed sound. When your nervous system is already overwhelmed, you start counting ceiling tiles just to feel like you’re doing something.
There was also almost nothing to do.
Some psychiatric units I had previously been in at least attempted therapeutic engagement through art, music, structured activities, or spaces that felt remotely human. This unit mostly revolved around eating meals, sitting around, and watching whatever happened to be on the communal television.
The group therapy sessions often felt equally hollow. Many were run by people who seemed to be working off simplified worksheets and canned responses rather than genuinely engaging with complex human beings. At times it honestly felt less like therapy and more like people reciting cliff notes about mental health to vulnerable patients trapped in the room.
And maybe that was the hardest part. Not just the discomfort, but the feeling that the system often mistakes management for care.
Yes, the healthcare system is overwhelmed in general, and psychiatric care is not somehow protected from that reality. In many ways, it may reflect the cracks in the system even more harshly because the people entering it are already emotionally vulnerable before they ever walk through the doors.
And sometimes psychiatric hospitalization honestly can feel less like deep treatment and more like emergency stabilization in an overcrowded system trying to keep up.
There are units where the goal genuinely seems to become: stabilize the immediate danger, adjust medications quickly, document improvement, free the bed for the next crisis waiting in the emergency room.
That sounds harsh, but I think most people who have spent significant time around inpatient psychiatric care understand exactly what I mean.
It does not necessarily mean the staff are evil or uncaring. Many are burned out, understaffed, emotionally exhausted, and working inside systems that were never given enough resources to handle the level of need coming through the doors every day.

But from the patient side, it can feel profoundly lonely.
You are sitting there during one of the hardest moments of your life while the institution around you is also functioning like a machine under pressure. Beds are limited. Time is limited. Staff attention is divided between people in completely different kinds of crises. And somewhere inside all of that, actual human healing is supposed to happen.
Sometimes it does.
Sometimes people leave safer, more stable, and genuinely helped.
And sometimes people leave feeling like they were processed through a system that was trying to manage risk faster than it was trying to understand them.
I eventually realized that, at least in that particular hospitalization, the primary goal no longer felt like truly understanding me or helping me improve in any meaningful long-term way. It felt like the system was trying to stabilize people quickly enough to free up beds in an overcrowded psychiatric unit.
And once I understood that, I understood the equation.
The system rewarded people who appeared calm, compliant, cooperative, and manageable. So that’s what I became.
I said the right things. I attended the groups. I avoided showing frustration. I learned which emotions raised concern and which responses signaled “progress.” And within days, I was discharged.
That realization was unsettling in its own way.
Because while some patients genuinely are improving during inpatient treatment, others are also learning how to perform improvement well enough to leave an environment that feels frightening, humiliating, or emotionally unsafe to them.
And that’s the part that still stays with me.
You do not have to be psychologically healthy to figure out how to get discharged from a psychiatric unit. You simply have to understand the equation.
In my case, leaving was probably the right thing. I understood that the environment was worsening my mental state instead of helping it, so I adapted, complied, performed stability, and got out within days.
But someone else could do the exact same thing for very different reasons.
A person in active crisis can also learn the script. They can learn what staff want to hear. They can learn how to appear calm, organized, optimistic, compliant, future-oriented. They can learn how to suppress what they are actually thinking long enough to satisfy the system’s requirements for discharge.
One patient “playing the game” may be advocating for themselves appropriately in a bad environment. Another may be dangerously unwell and simply masking effectively.
From the outside, both can look exactly the same.
What stays with you afterward is not always the hospitalization itself. Sometimes it’s the fear.
The fear that your mental health history can suddenly supersede every other fact about you. That once “psychiatric patient” enters your chart, it can begin coloring how people interpret your personality, your emotions, your reactions, your judgment, even your physical health concerns.
You start wondering whether people are hearing you clearly or filtering you through diagnosis first.
Are you anxious, or are you “irrational”? Are you frustrated, or are you “agitated”? Are you advocating for yourself, or are you being “difficult”?
That fear is hard to explain to people who have never experienced it. The feeling that once mental illness becomes part of your medical identity, there is always the possibility that your credibility becomes conditional.
And maybe that’s why the more humane psychiatric units mattered so much to me. The better staff never made me feel like my diagnosis erased my personhood. They understood that mental illness is something a person experiences, not the entirety of who they are.
To be fair, not every psychiatric unit feels cold or dehumanizing. That contrast is part of what makes all of this so complicated to talk about honestly.
I’ve been in units where staff treated patients with dignity. Places that actually attempted to create some sense of structure, engagement, and humanity beyond medication passes and observation checks. There were scheduled walks, art activities, music therapy, conversations that felt genuine, and moments where you could almost forget you were locked inside a psychiatric facility for a little while.
Those environments felt less like containment and more like recovery.
Even small things mattered. Staff remembering your name. Someone asking how you actually slept instead of just checking a box. Having activities that reminded you that your brain still deserved stimulation, creativity, and connection instead of just surveillance.
And then I’ve been in places that felt almost entirely custodial. Places where patients mostly wandered around waiting for the next meal, the next medication round, or the next shift change. Endless pacing. Television noise. Fluorescent lights. Nothing meaningful to engage your mind while you’re already trapped inside your own thoughts.
That difference matters more than people realize. Because boredom inside a psychiatric unit is not normal boredom. It eats at you in a specific way. Especially when you are already anxious, depressed, overstimulated, frightened, or mentally exhausted. Humans in crisis still need stimulation, connection, distraction, creativity, movement, and moments that remind them they are more than patients being monitored.
I don’t know what the right answer is. I know what helped me and what didn’t. I know some of those units treated me like a person and some treated me like a liability. And I know that distinction mattered more to my recovery than any medication adjustment or group therapy worksheet ever did.
I think you have done an outstanding job describing the dichotomy of psychiatric care in terms of helpful/relational vs intensifying fears and feeling inhumanized. There is something about being locked in a cage that brings out an animal fear and fury, too. A locked psych ward is very similar to a cage when someone is already having difficulties.